A Preliminary Look At Global Vaccine Outcomes and Lessons for Canada
Beata Caranci, SVP & Chief Economist | 416-982-8067
Sohaib Shahid, Senior Economist | 416-982-2556
Date Published: February 11, 2021
Highlights
- Vaccines are the cure to the stop-and-go economy that is pushing businesses to the edge. However, the experiences of Israel and the UK indicate that even when a more aggressive vaccine campaign gets off the ground in Canada, targeted restrictions will need to be maintained in the short run.
- Hospital capacity has been a key trigger for Canadian provinces to tighten restrictions. International experiences indicate that hospitalization stress related to COVID can be more quickly reduced by focusing vaccinations exclusively on the elderly and others most at risk of developing extreme disease.
- Until the elderly are vaccinated, anything that encourages gatherings of younger people should be managed carefully. Communities and groups that are at greater risk of spreading the virus should be the focus of higher frequency and accessible testing.
This time last year, we used China's economic experience as a guide into what to expect for Europe and North America, as the virus and business restrictions migrated across regions. Now, Israel and the UK offer insights for Canada into the degree to which a successful vaccination rollout can relax business restrictions and speed up the economic recovery.
Canada's vaccine rollout has been lagging other advanced economies. Unexpected shipment reductions have placed the month of March as a critical period for vaccine deliveries. Combined shipments of Moderna and Pfizer are expected to reach 3.1 million doses in March alone, compared to roughly 2.4 million doses that are expected to be delivered between the months of December and February.1
A smooth vaccine roll-out is a necessary condition for a sustained economic recovery, but it can follow many paths. Both the UK and Israel experiences indicate that even when there is speed and scale on the vaccination effort, business and social restrictions are slow to be removed. The presence of more contagious or detrimental variants of the virus are adding to the enhanced caution. For example, Israel and the UK imposed nationwide lockdowns a few weeks after their vaccine rollouts. Israel's restrictions ended on February 7, while the UK is expected to lift measures at the end of March. By the end of Israel's lockdown, it had vaccinated 40% of the population, while the UK will have vaccinated at least 35% of the population.
The lag between vaccination thresholds and an easing in restrictions is likely going to be an outcome repeated in Canada, where governments have demonstrated that the threat to hospital capacity is a key trigger to required restrictions. And, a more precarious supply of vaccines within Canada highlights the urgency to deliver with speed and precision.
Let's take Ontario as the example. Although elderly account for only 21% of the recent 2nd wave of virus cases, they make up roughly 69% of hospitalizations and 93% of fatalities. It's also been well documented over the past year that hospital stays are significantly longer for this age cohort. This suggests that the coupling of vaccine efforts and economic outcomes can be most effective with a focus exclusively on those at greatest risk of developing severe illness and hospitalization. Even after doing so, the lesson learned from Israel is that it takes time to reap the benefits from even the first dose of the vaccine.
In addition, restrictions may linger longer because vaccine outcomes are still being understood by the medical community. Israel's concentrated use of the Pfizer vaccine has demonstrated that it remains highly effective for the elderly, and its yet unclear the degree to which other vaccines will replicate this outcome. Canada should take care to ensure that those vaccines with strong, demonstrated outcomes for the elderly are prioritized for that group, particularly with supply far from assured from one month to the next
Canada's Vaccination Program Lags Its Peers
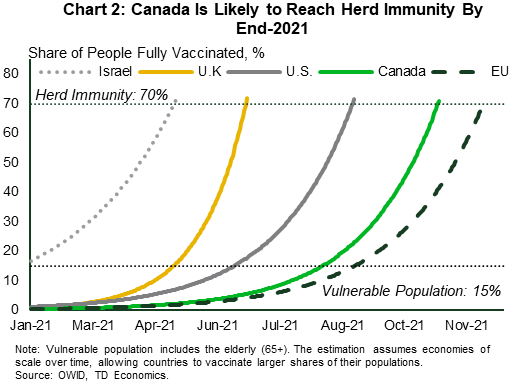
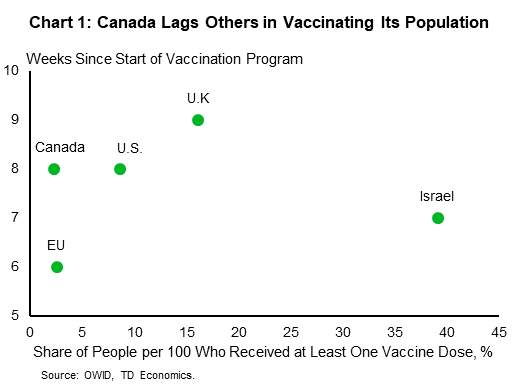
Canada was one of the first countries to authorize vaccines, but its rollout has been slower than peers (Chart 1). There are several reasons for the delays, from the typical growing pains other countries experienced related to the scaling up of a large and complex program, to the more recent obstacles stemming from interrupted and insufficient supply relative to other G7 countries. In two months, only 2.3% of the Canadian population has received at least one dose. If vaccine administration speeds up in the coming months as telegraphed by various government levels, we estimate it will still take until the end of 2021 to achieve herd immunity (Chart 2). You don't necessarily need herd immunity to move towards a normalization of the economy. But, you do need to create a sustainable model that mitigates pressures on hospitals and the society at large.
Early Lessons From Israel And the UK
Right from the outset, Israel's vaccination program has set an example for the rest of the world. It prioritized the elderly and vaccinated almost 40% of its population within 7 weeks. Around 90% of Israel's elderly population has already received the first dose, with 80% having received both doses. The UK is not too far behind with the first dose being received by 18% of its population and 90% of its over-80 population. However, due to their policy of delaying the second dose by 12 weeks, only 0.75% of the population has received full vaccination.
So how did Israel quickly vaccinate its population?
Price may have been a partial factor to securing vaccines, as some reports suggest Israel paid up for the Pfizer vaccine relative to other countries. However, Israel's more reliable supply may also reflect its ability to exploit a comparative advantage. The government promised to provide anonymized age, sex and demographic data of vaccinated people to Pfizer. In other words, Israel offered to work as a partner with Pfizer to build a stronger understanding of its vaccine efficacy and limitations on a scale much larger than could have been achieved in Stage 3 trials. In turn, this helps Pfizer course correct with greater speed.
This was made possible by Israel's strong health infrastructure and logistics. It also has a universal healthcare system in which each person has a digitised health record that facilitates tracking and communicating with patients. Lastly, its small geographical footprint – 6 times smaller than Southern Ontario – has also helped with the vaccine distribution and logistics. The UK has many of these same benefits.
Israel was also strongly motivated to seek a swift solution. It does not produce any of the approved vaccines, which sets it apart from the UK, which manufactures Pfizer, Moderna and Oxford-Astrazeneca vaccines. In addition, Israel has also spent the longest time in lockdown of any country, which created immense domestic pressure – the government collapsed in December 2020. It's not surprising that the new government made all efforts to receive accelerated access to the vaccine.
Israel is also not a federation in which sub-national governments are responsible for the provision of healthcare. Here too the UK draws similarities. These factors have made the coordination of vaccination efforts much easier. Notwithstanding some of these differences with Canada, there are lessons to be learned:
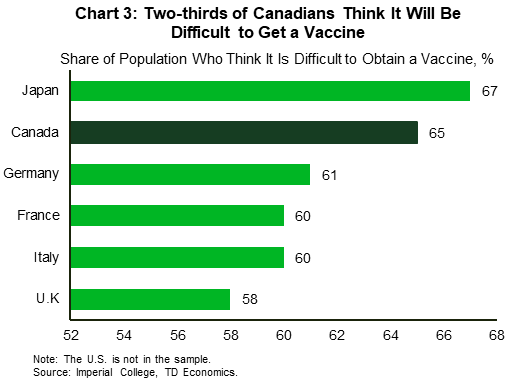
- Israel decentralized vaccine sites away from hospitals and into areas where accessibility might be an issue. This is especially important for Canada where its large geographic reach and population distribution can make it particularly difficult for the elderly and those at risk of developing severe illness to get vaccinated (Chart 3).
- Israel relied heavily on its military in vaccinating its population. The military's involvement allowed for a quick and efficient set up of inoculation sites.
- It did extensive community outreach and leveraged community-based health centres and institutions.
- Israel maintains a sense of urgency in its vaccination efforts by operating centres around the clock.
Are Israel and the UK's vaccination programs working?
Yes, but not as fast as some might prefer. Data from Israel show that those receiving one dose only had 33% fewer infections than those not vaccinated (unlike the 52% figure in clinical trials).2 But, the vaccine is 66 to 85% effective for those who received two doses.3 The vaccine is also 87 to 96% effective in stopping severe disease from the virus. This has a substantive impact on the health system and provides reassurance for vaccine efficacy. Not surprisingly, hospitalizations are falling in both Israel and the UK, but at differing rates. Compared to the mid-January peak, UK's hospitalization rates have come down 19% versus a 31% drop in Israel. The smaller drop in the UK may reflect a number of factors including the slightly lagged vaccination program, weaker efficacy of the single dose that was also seen in Israel, and the policy of delaying the 2nd dose. As yet, it is too soon to say what impact full vaccinations will have on UK's hospitalization rates.
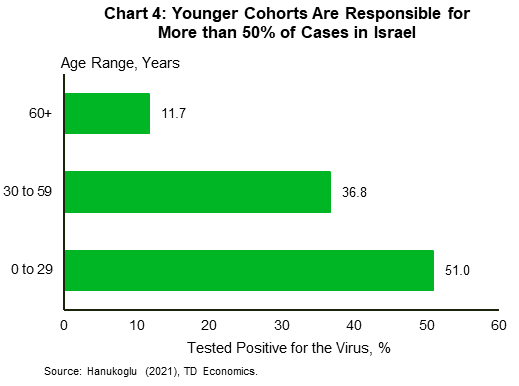
In Israel's case, hospitalizations started to decrease roughly 5 weeks after the start of its vaccination program on December 19. Keep in mind that at that time, Israel was already vaccinating at 10 times the rate of Canada. Even so, hospitalizations remain elevated relative to the Israeli government's comfort level. The more contagious UK variant is believed to be responsible for the still-elevated case loads, especially among the younger aged cohorts (Chart 4).4 In Israel, this variant is estimated to be accounting for roughly half of all cases, and it's conceivable that it could also become the dominant variant in Canada as more time elapses. Israel offers a cautionary tale of the need for speed on vaccinating the most vulnerable groups, while also maintaining some controls in place to limit the spread among other age cohorts. Although Israel lifted a month-long lockdown on February 7 – with over 40% of its population vaccinated with at least one dose – health officials were still warning against doing so. For Canada, under current vaccine availability, the population may not surpass that same mark until around August. Provinces with the potent combination of high population density and older demographics – such as Quebec and Ontario – could be more delayed.
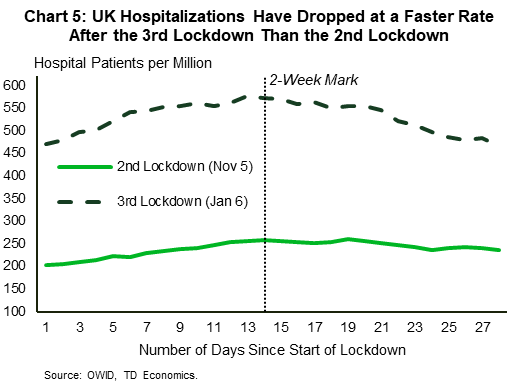
When Israel's cases first started falling after mid-January, it was difficult to say whether it was due to the vaccine or the lockdown. But, the latest data indicate that the decline (-46%) in cases among the elderly (the first in line for the vaccination) have been more pronounced than the decline (-18%) among the younger population. Since both the elderly and the young saw a similar decline during Israel's September lockdown, this means that the divergent drop in cases this time around can be attributed to the vaccine. Even in the UK, hospitalizations dropped slightly faster after the 3rd lockdown compared to the 2nd one (Chart 5). The divergent drop in hospitalizations between the 2nd and 3rd lockdowns – albeit milder than in Israel – is likely attributed to the UK's administration of the first dose.
That said, it's difficult to tease out with precision the direct effects. The divergence could also be partly related to behaviors. Those who were vaccinated first may also be more likely to exhibit cautious behavior due to their risks. We will only be able to 'cleanly' attribute the impact of the vaccine on new cases and hospitalizations roughly two weeks after the end of the lockdown and once those vaccinated can move about freely. For Israel that would be in the second half of February, while for the UK it could be as late as early-April.
Vaccines Are The Starting Point For Economic Recovery, But The Paths Can Vary
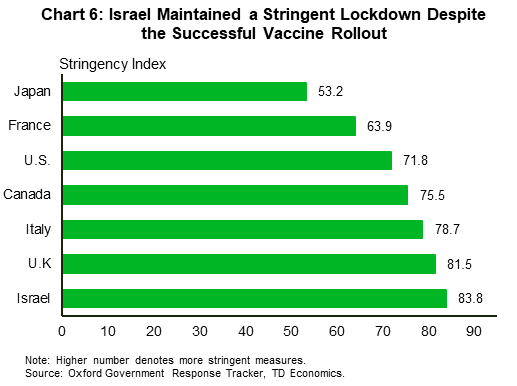
The path of economic recovery depends on the path of the virus, which in turn depends on the path of vaccine administration. A smooth and speedy vaccine roll-out is a necessary condition for a sustainable economic recovery that prevents the stop-and-go economic cycles of the past year. However, Israel's experience has shown that the benefits towards loosening restrictions will come with lags, and this, in turn, will depend on the ability to meaningfully influence severe illness and hospitalization rates. Throughout an aggressive and successful vaccination campaign, the country still maintained strict nation-wide lockdowns (Chart 6).
For Canada, vaccine supply issues layer on additional complexities, suggesting that timely, targeted and temporary restrictions would need to complement the vaccine efforts until several questions can be answered:
Impact of new variants: While some vaccines may be effective against some variants (for example Pfizer and Moderna against the UK variant), it doesn't necessarily mean that the vaccines will be effective against all existing and future variants, or that Canada will have timely access to those vaccines. This speaks to the necessary speed of Canada's vaccination program to limit the spread of more virulent variants within the most vulnerable portion of the population to severe illness.
Efficacy in the elderly: Most vaccine trials did not include (enough) elderly or those with underlying health conditions. While the Pfizer vaccine has been effective on both fronts, the same is not yet assured with other vaccines. Although the WHO recently endorsed the use of the Oxford-AstraZeneca vaccine, France, Germany, Italy, Sweden and Poland have advised against its use for older people, while Swiss medical regulators have disallowed its use altogether. Meanwhile, the Moderna vaccine has been shown to be less effective (86%) in older people compared to its overall efficacy (94%). However, this is still an extremely high efficacy rate and would materially reduce illness, hospitalizations and fatality rates.
Effect on transmission: The base case assumption is that the vaccines will prevent transmission. A vaccine's ability to prevent (or reduce) transmission will vary and none of the trials of the vaccines approved so far have drawn firm conclusions. From the rollout in Israel, we do not yet conclusively know whether vaccinated people are indirectly protecting unvaccinated people. Perhaps the case loads would have been lower if the Pfizer vaccine was preventing transmission to others? More time is needed to evaluate the data.

Vaccine skepticism: Vaccine skepticism remains high across the world. In January, 67% of Canadians showed a willingness to take the vaccine when made available.5 Digging into the details reveals that younger Canadians are less eager (55%) to take the vaccine compared to the elderly (73%) (Chart 7).6 Vaccine skepticism (in addition to slower supplies) among the younger population is one of the reasons Israel's vaccination rate dropped in recent days. It is important that at least 70% of a country's adult population is vaccinated to gain herd immunity.
Vaccine nationalism: We noted six months ago that there will be a lack of cooperation among countries when a vaccine comes onto the market (see our report). We also warned that "relying too much on imports for critical drugs and vaccines" can lead to possible shortages, for countries – like Canada – with insecure supply chains. We are seeing both trends today. A good example is the EU's recent decision to impose controls on vaccine exports to some countries. Although the EU has verbally reassured Canada that the policy won't be applied, circumstances are highly volatile. Governments are operating within pressure-cooker environments, and vaccine demand will far outstrip supply for months to come. Assurances can always prove fleeting if pressures continue to build.
Lessons For Policymakers:
1. Elderly first, others later
We know by now that the longer the lockdowns, the deeper the economic wounds. Businesses have been operating under degrees of lockdowns over the past year, and even with government support programs, the longevity of lockdowns does impact the odds of survivorship due to debt accumulation and other factors (see our report). But lockdowns cannot be eased if hospitalization stress remains high. And hospitalizations cannot ease if the elderly are contracting the virus. Therefore, given the limited vaccines and other associated risks, a vaccination program should focus exclusively on prioritizing the elderly and those most prone to being hospitalized. Such a program can also achieve a faster and more sustainable relaxation of business restrictions. Both Israel and the UK – two of the most successful vaccination programs – prioritized the elderly in the first phase of their vaccination programs.
Under the current approach, the benefits to the elderly and hospitalizations are being delayed, with a similar outcome on the timing of the economic recovery. The temporary freeze in Pfizer shipments was a major blow to Canadian provinces who scrambled to adjust their vaccination schedule to delay their second doses. Ontario, British Columbia and Alberta have delayed the second dose by up to 42 days. Meanwhile, Quebec has delayed the second dose by up to 90 days. With such a gap between the first and second doses, there will likewise be longer lags in Canada on a critical reduction in hospitalizations, thereby requiring stricter economic lockdowns than the counterfactual scenario.
Young people are less susceptible to being hospitalized, creating less of a burden on the health system relative to infection rates. However, the younger cohorts were the primary drivers of the virus' second wave last year. This suggests that high risk-factors will continue to exist even as the vaccination program matures within Canada. These should be carefully managed until the elderly and those susceptible to high hospitalizations have been vaccinated. One way of doing this is to ensure that the young and other high-risk groups become an increased focus for testing. These groups should be prioritized for highly accessible and/or frequent testing to stop the spread.
2. The need for speed
The faster that vaccines are rolled-out, the quicker that hospitalizations can drop on a sustained basis and the sooner we'll return to 'normal'. Israel is a good case in point. It fully vaccinated almost 80% of its elderly population in just 7 weeks, whereas the rollout among the under-60s began later and is climbing more slowly. As a result, there has been a 41% drop in cases in the elderly and a 31% drop in hospitalizations from mid-January to early-February. This is especially relevant for Canada where the elderly represent a higher share (18%) of the population, compared to countries with faster vaccination programs like the U.S. (15%) and Israel (12%).
3. Go with what you know
Given that Canada's vaccine supply chains are not secure, it is hedging its bets by securing orders from other vaccine makers such as Novavax (52 million doses) and Johnson & Johnson (38 million doses). However, the experience of Israel and the UK have reinforced that outcomes can change once vaccines are outside of a trial environment and being monitored within a large sample of elderly and people with comorbidities. If possible, Canadian governments could consider designating vaccines on the different population age cohorts that offer more predictable outcomes on hospitalization. In turn, this would have the added benefit of speeding up economic normalization and mitigating further permanent scaring on businesses and workers. However, this would need to be balanced against vaccine availability and the ability to achieve speed and scale of the vaccination program.Bottom Line
Vaccines are a necessary condition for economic recovery but won't immediately unlock Canada's full economic potential. Vaccination programs will need to remain coupled with targeted restrictions in the short run. The length of time of further business interruptions can be mitigated by focusing the vaccination programs on those individuals who bear the greatest risk of severe illness and hospitalization. And, until the elderly are vaccinated, anything that encourages gatherings of younger people should be managed carefully. With the lull in vaccine shipments and international examples offering new knowledge, now is the time for Canadian policymakers to retool. Canada stands at a critical juncture.
End Notes
- https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/prevention-risks/covid-19-vaccine-treatment/vaccine-rollout.html#a4b (data extracted on 8th February).
- Mahase, Elizabeth (2021), "Covid-19: Reports from Israel suggest one dose of Pfizer vaccine could be less effective than expected." BMJ 2021; 372:n217.
- Rossman et al. (2021), "Patterns of covid-19 pandemic dynamics following deployment of a broad national immunization program." Weizmann Institute of Science, Tel Aviv University.
- Hanukoglu, Israel (2021, February 08), "Coronavirus COVID-19: Age distribution of confirmed cases in Israel."
- https://www.imperial.ac.uk/media/imperial-college/institute-of-global-health-innovation/GlobalVaccineInsights_ICL-Covid-19-Behaviour-Tracker-EMBARGOED-00.01-04.02.2021.pdf
- http://angusreid.org/canada-covid-vaccine-january/
Disclaimer
This report is provided by TD Economics. It is for informational and educational purposes only as of the date of writing, and may not be appropriate for other purposes. The views and opinions expressed may change at any time based on market or other conditions and may not come to pass. This material is not intended to be relied upon as investment advice or recommendations, does not constitute a solicitation to buy or sell securities and should not be considered specific legal, investment or tax advice. The report does not provide material information about the business and affairs of TD Bank Group and the members of TD Economics are not spokespersons for TD Bank Group with respect to its business and affairs. The information contained in this report has been drawn from sources believed to be reliable, but is not guaranteed to be accurate or complete. This report contains economic analysis and views, including about future economic and financial markets performance. These are based on certain assumptions and other factors, and are subject to inherent risks and uncertainties. The actual outcome may be materially different. The Toronto-Dominion Bank and its affiliates and related entities that comprise the TD Bank Group are not liable for any errors or omissions in the information, analysis or views contained in this report, or for any loss or damage suffered.
Download
Share: